Shoulder Instability Treatment
The treatment for recurrent anterior dislocations is surgery.
The primary cause for ongoing shoulder instability is a tear of the glenoid labrum. Arthroscopically it is repaired back to the bone. Commonly three to four small anchors are inserted into the bone, securely reattaching the labrum. It usually takes about three months for healing to take place. However, the person needs to wait six months before returning to contact sport. In conjunction with labral repair, often other procedures need to be performed according to what is else has been damaged.
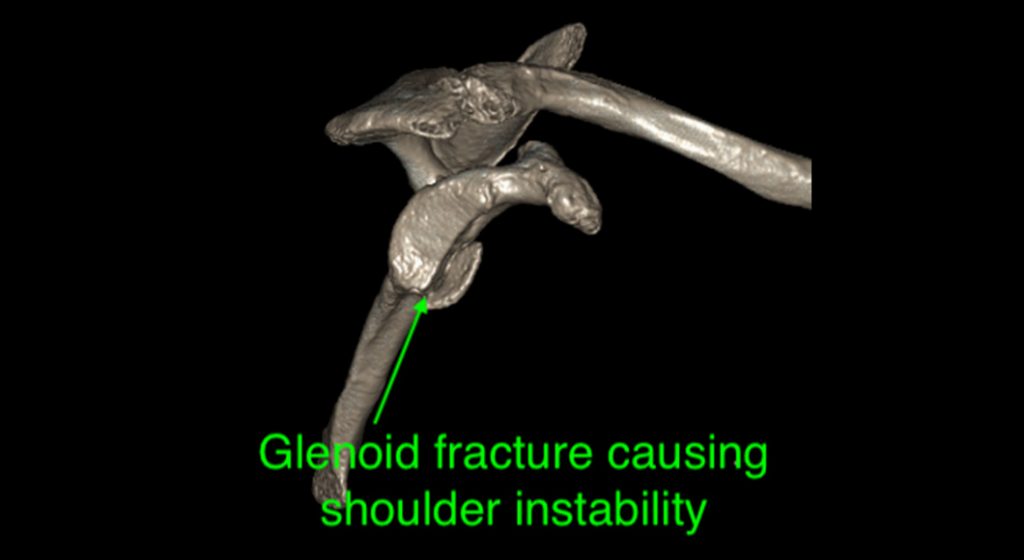
If significant bone loss occurs, a more extensive procedure is required. Bone loss may be due to a large fragment of bone (bony Bankart), breaking away at the time of the initial dislocation. However, bone loss can occur after many dislocations. Bone loss from the shoulder ball exacerbates this problem. In this situation, stability cannot be restored with a soft tissue procedure as described above. A bone graft procedure is required. The bone graft of choice is to take a nearby bone, called the coracoid process, and transfer it to the front of the socket where the bone loss has occurred. Two screws hold the graft. This operation is known as the Latarjet procedure. The advantage of taking the coracoid is that a tendon (the conjoined tendon) remains attached to the bone and it also improves stability by acting as a dynamic sling. It also has a good blood supply that enhances healing.
An ACL reconstruction involves reconstructing with a substitute tendon. The most common tendons used are the hamstring (semitendinosus), quadriceps or patellar tendons. The age of the patient and the sports played have a significant bearing on the best graft or tendon to use.

Dr Brown has successfully treated many patients with shoulder instability. After a thorough patient consultation, Dr Brown can recommend the most suitable non-surgical and surgical treatment to stabilise the shoulder.
Call us on (03) 5223 3151 Book an appointment today.
Posterior Dislocation
Posterior dislocations are far less frequent.
They usually occur with a fall onto the outstretched arm that drives the head of the humerus backwards. A posterior dislocation leads to tearing of the labrum from the back of the socket. Recurrent dislocations are less likely after a posterior dislocation. However, ongoing instability is managed by arthroscopic repair of the labrum.
Multidirectional instability
Often people with multidirectional instability suffer from generalised ligament laxity, and their shoulder instability is a manifestation of this. It also can occur in sports people like gymnasts and swimmers who put a lot of repetitive strain through their shoulders. Usually, the first line of treatment, if there has been no structural damage to the shoulder, is a thorough and extensive rehabilitation program. Rehabilitation involves a rotator cuff strengthening program and was well as strengthening the muscles that control the motion of the shoulder blade. Such a strategy needs to continue for at least six months. Avoidance of repetitive activities is necessary during this time.
For people who fail nonoperative treatment or if there is an underlying structural problem, they may require surgery. Typically the shoulder joint capsule and ligaments are stretched out. Arthroscopic surgery aims to “tighten” up the shoulder by placing multiple stitches through the capsule and in effect “double breasting” it. This operation is called a capsular plication. Postoperative rehabilitation again is extensive with the avoidance of aggravating activities for many months after.