Osteotomies around the knee are commonly performed procedures. “Osteotomy“ literally means “cutting of a bone”. Osteotomies are usually performed to correct deformities secondary to arthritis. The most typical deformity is a varus or “bow-legged” deformity. While a valgus, or “knock-kneed” deformity is less common.
The knee consists of basically two compartments: the medial or inner compartment and the lateral or outside compartment. Bodyweight is almost equally distributed between these two parts of the knee when performing weight-bearing activities. However, when the knee changes shape, more force is taken through the arthritic compartment, leading to activity-related pain. An osteotomy will redistribute the weight from the arthritic or diseased area and transfer it to the non-arthritic compartment. It is an excellent alternative to a knee replacement in younger and active people.
A high tibial osteotomy is a widely performed procedure to correct a bow-legged deformity due to arthritis, knee overload (secondary to meniscus removal), and knee instability. The goal of an osteotomy is to overcorrect the deformity by a small degree. There have been many techniques described to achieve this. The evolution of knee osteotomy is to create increasingly more accurate corrections.
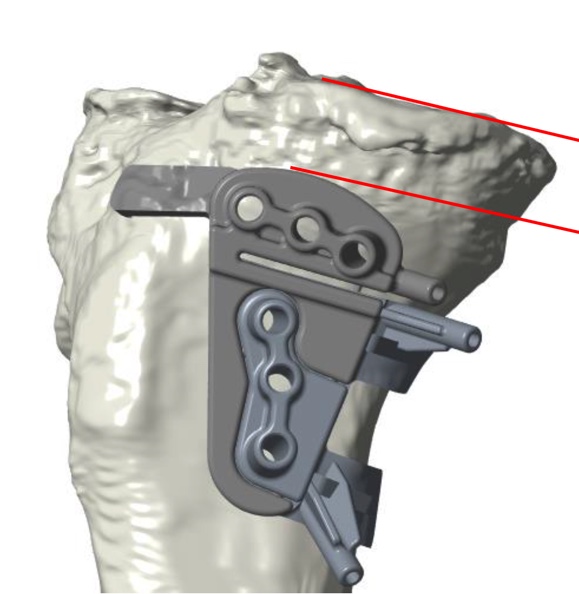
The latest development is the use of patient-specific guides. Here the person has a CT scan and X-ray of the knee, and engineers create a 3-dimensional model of the knee. I then decide on how much correction is required. A 3-D printer then creates the patient-specific guide. With a series of checks and double-checks, I can then perform a very precise osteotomy. A robust plate and screws then fixes the osteotomy, which is then bone grafted. This technique has made osteotomies more reliable and reproducible.