Knee pain affects many people every day. However, there are many different causes. This blog will discuss chronic (longer than three months) knee pain. As a surgeon, I was trained to make a diagnosis based on the patient’s history (the symptoms), my examination findings (the signs) and special tests, such as X-rays and MRI scans.
Each knee condition has a characteristic set of symptoms that include how the pain began, whether it’s worsening, the location, and those activities that may aggravate or relieve the pain. Similarly, each knee problem has different physical findings, such as limp, swelling, restricted movement, tenderness and, what we call, special tests. Therefore, if the pain pattern indicates a specific condition, correlated by my examination and confirmed by the imaging studies, I would be confident about the diagnosis. However, if there are discrepancies, then I would be less certain.
Many patients come to see me and tell me their MRI scan says they have a meniscus tear, for example. But if the symptoms and signs don’t match, the tear may be a “false positive”. It might appear that I’ve laboured the point, but making an accurate diagnosis is critical to good decision-making in surgery. Without it, the wrong treatment may be prescribed. And it doesn’t matter how good the surgeon is at operating; if an inappropriate or incorrect operation is performed, the patient won’t get a satisfactory outcome.
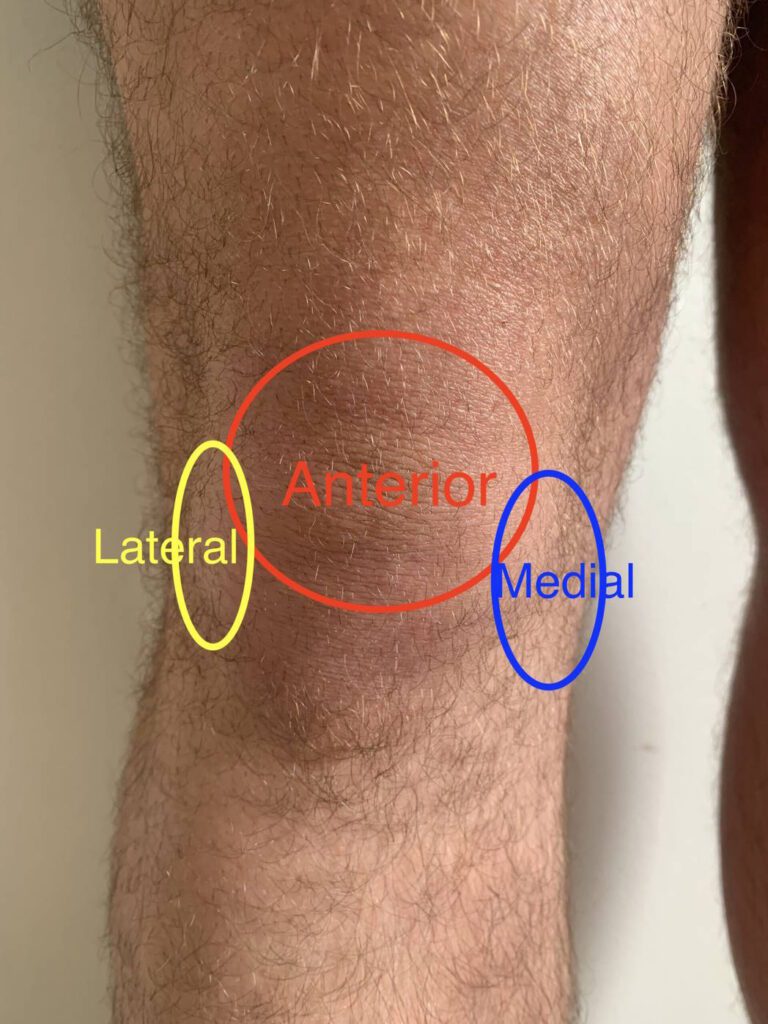
The location of the pain is critical in determining the cause of the pain. Pain in the front of the knee is prevalent and invariably arises from the knee cap. It occurs in three different age cohorts. The first is in adolescent (predominantly) females and is common. It generally responds well to a strengthening program. The next group is middle-aged individuals who may have lost condition and put on weight. They, too, respond well to strengthening and weight loss. The other group are those over 60 with arthritis of the patellofemoral joint. Kneecap pain is frequently superimposed on other knee conditions, often secondary to knee swelling and muscle loss.
Pain on the inside (medial) of the knee is also common. The pain is most commonly due to a meniscus tear in those under 50. For those over 60, arthritis is the usual cause. However, for those 50 to 60, there is considerable overlap, and younger people can develop arthritis. (For more details see our Meniscus Injury page and Knee Arthritis page).
Lateral knee pain (pain on the outside of the knee) is less prevalent, but the common causes are the same as for medial knee pain. For those under 50, think lateral meniscus tears; arthritis for older people.
Arthritis may be responsible for more generalised pain, including pain in the back of the knee. However, pain purely in the back of the knee is more unusual. It may be due to a Baker’s or popliteal cyst or a tear of the attachment point of the medial meniscus. Also, pain above and below the kneecap may indicate some specific conditions.
This list is not exhaustive, but the location of the pain is essential in making a diagnosis. Finally, some present with knee pain that is referred from the hip. This is uncommon but well-documented. I’ll finish with a story of a lady who came to see me with ongoing knee pain one year after her knee replacement. After three months, she realised that the pain was exactly the same as before the surgery. Examination of her hip and X-rays demonstrated an arthritic hip. Her knee pain resolved with a hip replacement.
So this is why you’ll be asked in detail about your pain. It’s best for me never to assume that an X-ray or an MRI gives all the answers.
For information on how to book an appointment with me, please visit our Appointments page.